
Case Report | DOI: https://doi.org/10.31579/2641-5194/043
*Corresponding Author: SULE Muhammad Baba, Department of Radiology, Usmanu Danfodiyo University, Sokoto.
Citation: Sule MB, Umar A.U., Gele I.H., Dada M.A, Ribah MM, Aliyu AZ, (2021 Radiologic Findings of Splenic Abscess: A Report of Two Cases. J. Gastroenterology Pancreatology and Hepatobilary Disorders. 5(5) DOI: 10.31579/2641-5194/043
Copyright: © 2021, Sule MB, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 10 August 2021 | Accepted: 25 August 2021 | Published: 07 September 2021
Keywords: spleen; abscess; volume; microbial; CT scan; HU=22
Splenic abscess is a very rare entity with an incidence of about 0.14-0.7% in autopsy studies. Splenic abscess has been reported to have a mortality rate of about47%, it has various causes but usually associated with trauma and infections of the spleen. We report two cases of splenic abscess; a child with post traumatic cause and a middle aged lady with an unknown cause.
Both cases were diagnosed of having the abscess following imaging; the first case had abdominopelvic ultrasound that showed an abscess cavity with a volume of about 11mls and subsequently resolved following medical treatment with intravenous antimicrobial agents. The second case however had an abdominopelvic computed tomography scan that showed a huge splenic abscess with a volume of about 1400mls; she had a successful splenectomy. We report the radiologic findings of these cases due to the rare nature of splenic abscess as reported in the literature.
Splenic abscess is a very rare entity with an incidence of about 0.14-0.7% in autopsy studies [1-4]. Splenic abscess though been rare, they show changing patterns of diagnosis and treatment [4]. Splenic abscess has been reported to have a mortality rate of about47%, it has various causes but usually associated with trauma and infections of the spleen [5, 6]. The incidence of splenic abscess shows an apparent increase most likely from advances in imaging studies and an increased number of immunocompromised, trauma and cancer patients [5, 7, 8]. Infective causes are the leading cause of splenic abscess, the two main contributing organisms responsible for most cases of splenic abscess are Klebsilae pneumonia and Streptococcus [4, 5]. The most common cause of splenic abscess is from hematogenous spread, and typically arise from endocarditis or seeding from some contiguous sites of infection [9, 10]. Splenic abscess is associated with some risk factors, among which are immunocompromised status, hemoglobinopathies and diabetes mellitus [1, 11]. The diagnosis of splenic abscess can be done early by combination of computed tomography, abdominal ultrasonography and clinical features [1, 3, 11-15]. Splenic abscess can mainly be managed by medical therapy, percutaneous aspiration (CT-guided and Abdominal ultrasonographic-guided) and splenectomy [15].
Case 1
This is a ten-month-old infant who was referred for Abdominopelvic ultrasound following a history of fall, left hypochondrial pain, chills and rigor with easy irritability. His genotye is AA type and has no retroviral infection. The patient had tender splenomegaly at the time of presentation.
The cardiovascular and respiratory systems evaluation were all within normal limits. He had much tenderness to sonographic probe pressure over the left hypochondrium.
The abdominal sonogram showed splenomegaly with a well circumscribed area of echogenicity with peripheral reduced reflectivity was demonstrated; the volume of which was 11mls following which a diagnosis of an abscess cavity in the spleen was made (figure 1). A plain abdominal x-ray showed sentinel loops with air fluid level in the left hypochondrium apart from the fundal gas. No history of immunosuppression was documented. The blood and abscess microscopy, culture and sensitivity yielded no growth. The blood film showed leukocytosis.
The patient got better with the use of intravenous broad spectrum antibiotics (Augmentin and intravenous metronidazole) with analgesics. He was discharged from the hospital twenty-two days later.

Case 2
This is a 20-year-old female who was referred for Abdominopelvic computed tomography (CT) following history of recurrent left hypochondrial pain, chills and rigor with easy irritability for almost four weeks. Her genotye is AA type and has no retroviral infection. No history of fall or trauma and blood transfusion. The patient had non-tender splenomegaly at the time of presentation.
The cardiovascular and respiratory systems evaluation were all within normal limits.
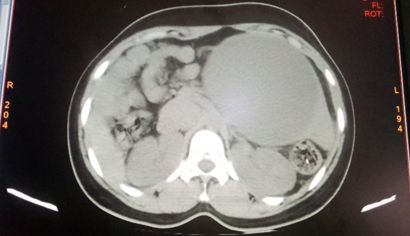
The CT scan showed an extensive well circumscribed area of non-enhancing iso-density (HU=22) with a volume of about 1400mls within the substance of the spleen. It showed no debri, loculation or septum. No any other similar collection was demonstrated within the spleen; (see figures 2 a and 2 b).
The blood and abscess microscopy, culture and sensitivity yielded no growth. The blood film showed leukocytosis.
The patient had initial intravenous broad spectrum antibiotics with subsequent splenectomy and got better afterwards, she was discharged home after three weeks.

Splenic abscess is a rare entity and usually may follow a traumatic scenario, infective or idiopathic course. The first case had a history of trauma while the second has an idiopathic scenario. The usual complaints documented in the literature are left hypochondrial pain and discomfort, fever, chills, loss of appetite and easy fatigability to mention a few; both cases presented here had such presenting complaints respectively. Splenic abscess has equal sex distribution, the cases we had were both male and female; these cases had solitary abscess cavity though with different volumes.
Patients with splenic abscess often do have a positive growth following blood and abscess culture respectively, only in a minor cases do the culture becomes negative. Both cases presented here had no growth following culture of both blood and abscess aspirates.
Splenic abscess may be associated with other intra-abdominal abscesses especially in the liver as documented following Typhoid splenic abscesses, the two cases presented here had no any other abscess in the liver or other abdominal organs. It is documented in most literatures that splenic abscess do have a higher morbidity and mortality rates, the first case had painful and agonizing pain and longer period of debility, both cases had a favorable outcome with no mortality recorded.
Some of the literatures showed better prognosis with antimicrobial agents for single and small volume abscess cavities while splenectomy was reported to be the suitable treatment option for larger volume and multiple cavities; similar findings were documented as the first case with a smaller volume of about 11mls did well on antimicrobial treatment while the second case with a larger volume of about 1400mls had splenectomy.
Splenic abscess is indeed a rare entity, basic imaging and clinical features are necessary in confirming the diagnosis early to save the life of the patients. The management can either be medical or splenectomy depending on the volume and nature of the abscess with the clinical presentation of the patient.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
